
Every year on 5 May, health facilities mark World Hand Hygiene Day. For AMCE, this year’s message is not distant or ceremonial. It is about what happens in the few seconds before we touch a patient, handle a line, adjust a catheter, examine a wound, move between bed spaces, or enter the next clinical task. Hand hygiene is not complicated, but it depends on a real decision made many times a day: stop, clean your hands, and protect the person in front of you.
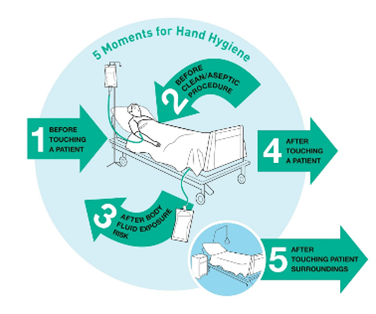
These five moments apply in every AMCE clinical area: the Oncology ward, Transplant unit, Dialysis centre, ICU, theatres, inpatient wards, outpatient clinics, pharmacy, and laboratory. The standard does not shift depending on how busy the unit is.
Why this matters here
Most hospitals do not transplant organs or treat haematological malignancies. AMCE one does.
The patients at AMCE are not a general hospital population. Many are profoundly immunocompromised: on active chemotherapy, recovering from haematopoietic stem cell transplantation, dependent on central venous catheters, or on long-term immunosuppressive drugs. For this group, a healthcare-associated infection does not mean a few extra days in hospital. It can derail a transplant course, force a pause in cancer treatment, progress to sepsis, or leave the clinical team with fewer antibiotic options than they had before.
In some cases, it costs a life that the whole team has worked hard to protect. |
Organisms that move through missed hand hygiene
- Carbapenem-resistant Gram-negative bacteria
- Meticillin-resistant Staphylococcus aureus
- Vancomycin-resistant enterococci
- Candida spp. with reduced azole susceptibility
None of these organisms announce themselves. A lapse in a corridor, at a nursing station, or during a brief bedside contact can be enough. The AMS and IPC programmes at AMCE exist partly to track where those lapses are happening.
Barriers to compliance
It is rarely a knowledge problem.
Most staff who miss a hand hygiene moment are not unaware of the requirement. The ward was busy, the dispenser was across the room, the moment passed. AMCE’s IPC rounds and ward audits will keep monitoring for these gaps. Dispensers must be in reach. Alcohol-based hand rub and soap must be stocked. If supplies are not where staff need them, that is an operational failure, not a staff failure.
One point worth stating plainly: gloves do not replace hand hygiene. A gloved hand picks up and transfers organisms just as an ungloved hand does. Hand hygiene before gloving and after removing gloves is still required. Both steps. This is not pedantic – it is where transmission happens.
Patients and families
“Have you cleaned your hands?”
A patient or visitor who asks that is not being obstructive. They are doing exactly what a safety-conscious unit should make comfortable. Staff who receive that question defensively are the problem, not the patient.
A unit where a patient can ask that question without hesitation is a unit where transmission risk is lower. It takes time to build. It gets undone fast if staff respond badly once.
Clean hands. Right time. Every patient.
AMCE holds this standard on World Hand Hygiene Day and on every other day of the year.